
Consultation Paper
CP19/23**
July 2019
Signposting to travel insurance for consumers
with medical conditions

2
CP19/23
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
How to respond
We are asking for comments on
this Consultation Paper (CP) by
15 September 2019.
You can send them to us using
the form on our website at:
www.fca.org.uk/cp19-23-response-form
Or in writing to:
Hannah Regan
Consumer Strategy & Policy
Financial Conduct Authority
12 Endeavour Square
London E20 1JN
Email:
signpostingtotravelinsurance@fca.org.uk
Contents
1 Summary 3
2 The wider context 7
3 Signposting rules and additional guidance 9
Annex 1
Questions in this paper 15
Annex 2
Annex 3
Compatibility statement 28
Annex 4
Abbreviations used in this paper 32
Appendix 1
Draft Handbook text
Search
How to navigate this document
returns you to the contents list
takes you to helpful abbreviations
takes you to the previous page
takes you to the next page
prints document
email and share document

3
CP19/23
Chapter 1
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
1 Summary
1.1 We want to help consumers with pre-existing medical conditions (PEMCs) who can
sometimes struggle to access affordable travel insurance that covers their conditions.
This consultation sets out our proposals for doing this and we are asking for your views.
Why we are consulting
1.2 We propose introducing measures to help consumers better navigate the market and
find firms that can offer travel insurance products that cover their PEMCs, and we
would like input from our stakeholders on these proposals.
Who this applies to
1.3 This consultation will be of interest to:
•
agents, intermediaries, and appointed representatives¹
•
• insurance industry trade associations
• charities, in particular medical charities
• consumer organisations
• consumers, primarily those with PEMCs
The wider context of this consultation
1.4 Over the past four years we have worked on issues affecting vulnerable consumers
and access to financial services. We have found that consumers with PEMCs can
sometimes face problems navigating the travel insurance market and finding
affordable cover for their conditions.
1.5 In June 2017, we issued a Call for Input (CfI) to gather further evidence. We focused on
those consumers with, or recovering from, cancer.
1.6 In July 2018, we outlined the feedback we received to the CfI. This indicated that
consumers with more serious PEMCs can struggle to identify firms that can provide
affordable cover for their PEMC. Consumers often give up their search after their
initial unsuccessful attempts. In some cases, this is because their application for travel
insurance is declined. Others are offered a policy containing exclusions for PEMCs or at
what they consider to be an unreasonably high premium.
and banks), and appointed representatives
Search

4
CP19/23
Chapter 1
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
1.7 This means some consumers are travelling without cover for their PEMC, cancelling
trips or paying significantly more for policies than they could with alternative firms.
Issues were prevalent across all PEMCs, not just cancer.
1.8 Nearly all consumers with a PEMC can get cover if they are able to find the right
provider. And often, if they can, the premium may also be more affordable. We know
it can be challenging to navigate the market to find more specialist providers. So we
have mainly looked at helping consumers effectively navigate the market and access all
providers.
1.9
purchase travel insurance each year. Of these consumers, approximately 0.7% were
declined cover, and 11% bought a policy that excluded their PEMC (see table 1 in Annex
2- Cost Benefit Analysis). A proportion of consumers who are offered a policy may
benefit from shopping around to find more affordable cover with a different provider.
We are unable to estimate the number of consumers in this group.
1.10 Since issuing the feedback statement, we have engaged extensively with stakeholders
through bilateral meetings and larger roundtable events. This has helped us to explore
the options available, test our proposals and establish a viable package that we believe
addresses the harm in a proportionate and practical way. We recognise that industry
and trade associations (such as BIBA and the ABI) have been engaged with this issue,
but our proposals aim to bring greater consistency across the industry.
What we want to change
1.11 This consultation seeks views on the following proposed changes to our Handbook:
•
to cover consumers with more serious PEMCs. The content and controls around
the directory will be developed by the FCA with the intention that the directory will
be hosted by the Money and Pensions Service (MAPS).
•
PEMCs
1.12 We are also looking to introduce a package of proposals to work together to achieve
optimal outcomes for consumers. We will work with:
• MAPS to improve consumer understanding of travel insurance policies for those
reiterate the importance of insurance; and
• our stakeholders to improve the wording used in the medical screening process,
aiming to make the process as easy as possible for consumers
1.13 These additional supporting remedies are discussed in more detail in 1.21 – 1.22 below.
Search

5
CP19/23
Chapter 1
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Outcomes we are seeking
1.14 We want to improve the travel insurance market by helping consumers with PEMCs
have better access to travel insurance products that cover their conditions. Our
proposals aim to increase consumer confidence and trust in the travel insurance
market by reducing the number of:
• consumers who feel frustrated and unable to navigate the market
• uninsured consumers, who are currently faced with a choice of not travelling or
running the risk of incurring significant costs, including medical bills, abroad
• consumers with PEMCs who are over-paying significantly for travel insurance
Measuring success
1.15 If we introduce these proposals, we will evaluate their impact using a range of evidence.
1.16 We will get feedback from stakeholders, including consumer organisations, charities
and consumers themselves, which will be extremely valuable in measuring the success
of the proposals. However, we have limited baseline data to give us an overview of how
the market is operating currently for consumers with PEMCs. This will make it difficult
to measure the success of the proposals against the current position in quantitative
terms.
1.17 We will work with MAPS to establish ways to collect data from the directory to show not
only how many consumers use the directory, but also the outcomes after using it. We
will also use information from our supervision of firms, including product governance
processes. These give insight into how travel insurance products reach their target
market and perform.
Next steps
Consultation
1.18 We are seeking your views on the proposals in this paper. Please send your comments
to us by 15 September 2019 using the online response form or by writing to us at the
address on page 2.
1.19 We will consider the feedback and publish a Policy Statement with our response to the
consultation feedback along with final rules, subject to responses to this consultation.
Supporting proposals
1.20 To complement the proposals that we are consulting on in this paper, we will work with
MAPS and our other stakeholders on 2 additional initiatives:
1. Consumer information
1.21 We want to ensure that consumers have access to relevant information to make
better informed decisions. We will work with stakeholders to try to improve consumer
understanding of the travel insurance market and will work with MAPS to produce
Search
CP19/23
Chapter 1
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
material for consumers with PEMCs. This will help consumers understand the
implications of travelling with exclusions, and how factors such as the country of
destination can affect medical costs and so affect travel insurance premiums.
2. Medical screening
1.22 Some of the wording used in the medical screening process² can be outdated
and uncomfortable for consumers to respond to, and there may be other ways of
wording questions that would still add value to the risk assessment. We are working
with stakeholders to decide how to improve this. We are working collaboratively with
charities and consumer organisations, as well as the medical screening companies.
Other related FCA work
1.23 The responses to our CfI highlighted some other concerns from our stakeholders in
relation to pricing practices within general insurance. While our proposals do not focus
on these concerns or this specific feedback, we are conducting other work on pricing
practices, the outcomes of which may be relevant to the travel insurance market:
• Our launched a debate on
assessing the fairness of a given pricing practice. Our approach here will apply to all
feedback statement later this summer.
• We are also conducting a General insurance pricing practices market study into how
existing and new consumers are charged for motor and home insurance and plan
health, pet and travel insurance are not included in the scope of the market study.
But, where possible, we will identify lessons from this study that are relevant to
other markets that we regulate, including travel insurance.
if the consumer may have a PEMC. If the answers to this/these questions indicate that they may have a PEMC, the consumer is
Search

7
CP19/23
Chapter 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
2 The wider context
The harm we are trying to reduce/prevent
2.1 Our work has identified 2 key issues for consumers:
• Access
capability and appetite to cover more serious PEMCs are often not on price-
policies with high premium rates can lead to consumers believing it is not possible
• Understanding – feedback from our stakeholders has shown that consumers may
quoted premium. We have also seen a general lack of understanding around the
impact of PEMC exclusions. This can result in consumers buying policies without
understanding the extent of their cover and/or feeling unfairly treated. A broader
lack of understanding of the market can also result in a lack of access to the entire
range of travel insurance providers available.
How it links to our objectives
Consumer protection
2.2 Our proposals are intended to protect consumers with PEMCs by reducing the number
of uninsured consumers, those with PEMC exclusions, and those who are unable to
access affordable insurance that covers their conditions. We aim to protect these
consumers from potentially having to pay large costs, including medical costs.
Market integrity
2.3 Our proposals aim to increase consumer confidence and trust in the travel insurance
market, with more consumers better able to find appropriate insurance cover for
Wider effects of this consultation
2.4 Annex 2 sets out our analysis of the associated costs and benefits to both firms and
consumers from our proposals.
2.5 Our proposals may also promote competition between travel insurance firms by
improving consumer access and awareness, increasing their ability and propensity to
shop around.
Search

8
CP19/23
Chapter 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Equality and diversity considerations
2.6 We have considered the equality and diversity issues that may arise from the proposals
in this Consultation Paper.
2.7
ability to carry out normal day to day activities.
2.8 The proposals are designed to assist consumers who have, or have had, PEMCs
to access travel insurance products that cover their conditions. This will include
consumers who are classed as disabled under the Equality Act, as well as many
PEMCs that are not considered a disability under the Act. Our proposal to improve
consumer understanding in this market also aims to assist consumers with PEMCs.
These proposals are intended to equip consumers with relevant information and help
them make more informed decisions, and to improve the process of buying insurance,
reducing unnecessary distress throughout the journey.
2.9 Overall, we consider that the proposals will positively impact the groups with protected
characteristics under the Equality Act 2010. However, we recognise that there is a risk
that the directory could be overwhelming to some consumers who use it, many of
whom will be vulnerable. We will work with MAPS to minimise this risk when developing
the directory.
2.10 We will continue to consider the equality and diversity implications of the proposals
during the consultation period, and will revisit them when making the final rules.
Search

9
CP19/23
Chapter 3
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
3 Signposting rules and additional
guidance
3.1 We are consulting on changes to our Handbook designed to make it easier for
consumers with PEMCs to access affordable travel insurance that covers their
conditions.
3.2 We are proposing:
1.
This directory will have the content and controls set by the FCA but the intention
is that it will be hosted by the Money and Pensions Service (MAPS). There is more
detail about this in paras 3.32-3.39.
2. Additional guidance to our existing rules, including on:
a. communicating with consumers about travel insurance policies with exclusions
for PEMCs and
b.
results of those assessments and/or the resulting premiums to consumers.
Signposting rule
3.3 We propose requiring all firms to give details of the directory to consumers that notify,
or have previously notified, a firm of a PEMC, in the following circumstances:
• Declines:
cover cancelled mid-term, due to a PEMC.
• Exclusions:
cannot be removed.
• Additional premiums:
loading³ to their base premium due to their PEMC.
3.4 The requirements would apply across all types of consumer journey (online, telephone,
or by other means) and to all firms providing or distributing retail travel insurance to
consumers in the UK
4
. If a consumer cannot access the internet, the firm must give
them a hard-copy version of the directory.
Additional premiums
3.5 We want to make sure that details of the directory are given to those consumers who
will most benefit from further shopping around and not those who are unlikely to
benefit.
3 An additional loading is a cost built into the insurance premium to cover additional risk that the insurer will suffer losses during the
period of cover.
4 Subject to any Directive restrictions.
Search

10
CP19/23
Chapter 3
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
3.6 If a consumer has been declined cover, or received a quote with a PEMC exclusion,
further shopping around is clearly likely to be beneficial. But if they have a quote
including cover for their condition, further shopping around will not always help. For
some, shopping around could result in a significant reduction in premium, while for
others, the initial provider may offer the best rates.
3.7 It is difficult to identify a trigger point for disclosing the directory information that
is both proportionate for firms to implement and which maximises getting the
information to those consumers most likely benefit, reducing consumer harm to the
greatest extent. We are proposing that all consumers with an additional loading to their
premium are notified of the directory. We considered the following options, some of
which were suggested by our stakeholders, for triggering the notification:
a. A medical screening score threshold, above which the notication is triggered.
This provides an objective test to trigger the disclosure. Also, the severity of a
new entrants to the market.
b. A premium amount threshold, above which the notication is triggered.
(a) in deciding on an appropriate threshold. Some stakeholders suggested that
signposting could be triggered at the price point above which only a very small
of consumers, then they should consider if they are meeting their wider regulatory
c. All consumers who declare a PEMC are notied. This also provides an objective
test, but would capture a large number of consumers who have no loading to their
premium (approximately 12% of those medically screened go on to receive no
additional loading, and a further 27% get a very low screening score and so could be
d. All consumers who receive an additional loading to their base premium, due to
a PEMC, are notied.
implement. It should also ensure that the disclosure is made to those consumers
shopping around further. But, on balance, we believe that this is the best option.
3.8 We want to limit the risk that consumers with a minimal loading (often due to a very
we propose that when signposting the consumer to the directory, firms indicate which
consumers are more likely to benefit from using it and state the potential benefits
of accessing it. They can explain it is likely to be more helpful for consumers with
condition.
Search

11
CP19/23
Chapter 3
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
3.9 We are aware this could put some onus on the consumer to decide whether their
believe the notification will help consumers to understand whether it may be of benefit
to them to access the directory rather than remain on their existing journey.
3.10 If the firm cannot ascertain whether premiums carry an additional loading due to a
PEMC it must disclose the details of the directory to consumers anyway.
Renewals and packaged bank accounts
3.11 Around 78% of policies sold are annual multi-trip policies (ABI, Mintel). Consumers can
choose to purchase another annual policy with another provider but often continue
with the same provider at point of renewal.
3.12 Packaged bank accounts (PBAs) are one of the most common ways of obtaining travel
blanket exclusion for all PEMCs. Consumers can go through medical screening, which
could result in the exclusion being removed. This might result in an additional loading to
the premium depending on the severity of the condition.
3.13 We are proposing that, for annual policyholders and PBA consumers, if a PEMC has
been declared leading to an additional premium or an exclusion (or if a blanket PEMC
exclusion has been applied and cannot be removed), firms must disclose details of
the directory. If an exclusion has been applied to a policy, regardless of the consumer
declaring any medical conditions, then the firm should disclose to the consumer
whether it can be removed from the policy, and if so, how it can be removed.
Existing industry initiatives
3.14 We are aware there are already many industry initiatives, and more still being
developed, to help consumers with PEMCs. These include firms referring consumers
with PEMCs to more specialist firms and other signposting.
3.15 Our proposals aim to introduce a consistent minimum standard for consumers across
the whole industry. But we welcome and encourage additional arrangements to
help consumers. Supplying details of the directory does not stop firms innovating to
improve the process.
3.16 Whilst we welcome industry initiatives, we are reminding firms of their obligations
under competition law. These include not disclosing any commercially sensitive
information to competitors such as pricing or price planning, customer or market
information or company strategy.
3.17 If firms refer consumers to one or more specific firms as well as providing them with
information about the directory, they should ensure that they comply with Principle 7
(Communications with Clients). This is to make sure that the status and utility of the
directory is made clear and consumers are not misled into believing the specific firm(s)
they are referred to is the only or best option available. It is also important for firms to
satisfy themselves that they are complying with Principle 8 (Conflicts of Interest) and
our rules, including ICOBS 2.2.2R, ICOBS 2.3, ICO BS2.5-1R and, where applicable, SYSC
19F about the arrangements they have with any specific firms they refer consumers
to. Firms should also ensure they comply with competition law requirements, in
particular the sharing of non-public information.
Search

12
CP19/23
Chapter 3
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Additional guidance
Exclusions
3.18 Some consumers may be buying policies with PEMC exclusions without being made
awareness of their options.
3.19 Our rules already require firms to disclose ‘appropriate information about a policy … so
Information Document, information about the main exclusions where claims cannot
3.20 We propose to introduce guidance that firms selling travel insurance policies that
exclude PEMCs should tell consumers whether and how PEMC exclusions can be
removed. This applies to new and existing consumers. Existing consumers should get
this information in their renewal notice or annual PBA eligibility statement.
High premiums
3.21 Stakeholders have suggested that consumers with PEMCs can sometimes receive
very high quotes from a provider.
3.22
happen if the firm lacks the experience or expertise to assess the risk accurately. It
may be better for consumers for firms not to offer a quote in those circumstances
and explain to consumers why a quote is not being provided. We also query whether
quote, they should provide an explanation to the consumer and details of the directory.
3.23 Consumers who receive very high premium quotations may incorrectly assume they
are unable to get affordable travel insurance due to their condition. Firms should
consider whether it would be fairer and more beneficial for the consumer to not offer a
quote and explain why.
3.24 Under PROD 4, products must be designed for an identified target market.
Manufacturers may identify groups of consumers for whose needs, characteristics
and objectives the insurance product is generally not compatible (PROD 4.2.18).
Furthermore, where firms distribute products that they do not manufacture they must
have adequate arrangements to understand the characteristics and identified target
market of each product (PROD 4.3.2).
3.25 We propose to add guidance saying that where firms offer cover to some consumers
at very high premiums, they should consider to what extent this is because those
consumers fall outside their target market. We expect those firms to consider whether
their offer is very expensive and may mislead the consumer, deterring them from
shopping around further. Alternatively, firms should consider whether their offer is very
expensive due to their lack of experience or ability to assess the risk in a way that will be
fair and beneficial to a consumer. The guidance will set out our expectations that:
Search

13
CP19/23
Chapter 3
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
•
•
requirements referred to above
3.26 In both circumstances, firms should consider whether not offering a quote would be
should also explain to consumers why they are not giving a quote.
Equality Act 2010
3.27 Firms are also reminded of their obligations under the Equality Act 2010, in
circumstances where the PEMC would amount to a disability under that Act.
3.28 There is an exception to certain prohibitions against disability discrimination in the
Equality Act that allows insurers to differentiate prices based on the risk that different
consumers present, where it is reasonable to do so. Firms are reminded that this must
be based on relevant and reliable information.
Demands and needs
3.29 We are concerned that some consumers with PEMCs take out travel insurance which
excludes cover for their condition.
3.30 Firms are reminded that, when proposing a contract of insurance, they must ensure it
ICOBS 5.2.2BR).
3.31 Where a firm is dealing with a consumer with a PEMC and proposes a policy which
excludes cover for that PEMC, the firm should consider how this meets its obligation
Directory
3.32 We propose to require firms to signpost consumers to a directory that:
•
provide insurance policies for consumers with more serious PEMCs
•
•
informed initial selection about which might meet their needs
•
3.33 We are working closely with MAPS on the development of the directory, with the
intention that it will be hosted on its website.
Search

14
CP19/23
Chapter 3
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
3.34 To be featured in the directory, firms will have to answer a series of questions
confirming that they have the appetite and screening capability to provide insurance
policies for consumers with more serious PEMCs. The FCA and MAPS will carry out
an initial joint validation process. To ensure that the information on the directory
information is kept up to date.
3.35 Consumers could also be referred to the directory by other organisations such as
charities and consumer bodies.
3.36 Information displayed on the directory should be broad enough to be useful for
consumers, but succinct enough to not be overwhelming. Suggestions for display are:
•
•
•
• any age limits
•
phone
•
treatment
•
3.37 There will be user testing of the directory, to ensure the format is practical and user-
friendly.
3.38 Firms which enter the market after the directory is in operation will be eligible for
inclusion if they satisfy the validation process.
3.39 There will be an opportunity for firms to submit applications to be listed on the
directory. We expect a relatively small number of firms to apply to be listed. We will
publish details of how to apply following the result of our consultation.
Implementation period
3.40 We propose to give firms 3 months to implement any changes from the time the rules
are made, by which time we expect the directory to be available.
Search

15
CP19/23
Chapter 3
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Annex 1
List of questions
Q1: Do you agree with our signposting proposals?
Q2: If you disagree, what would be your proposed approach
and why?
Q3:
Do you agree with our proposal for the trigger points for
disclosure for consumers with PEMCs?
Q4:
If you disagree, what would be your proposed approach
and why?
Q5:
Do you agree with our proposed guidance on exclusions?
Q6: Do you agree with our proposed guidance on high
premiums?
Q7:
Do you agree with our proposals for the directory?
Q8: What do you think is an adequate time to implement the
rule changes after we publish our nal rules and policy
statement, and why?
Search

CP19/23
Annex 1
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Annex 2
Cost benefit analysis
Introduction
1. FSMA requires us to publish a cost benefit analysis (CBA) of our proposed rules.
Specifically, it requires us to publish an analysis of the costs and benefits we expect will
arise if our proposed rules are made and an estimate of those costs and benefits.
2. However, FSMA also provides that if the costs or benefits cannot reasonably be
estimated or it is not reasonably practicable to produce an estimate, then we need
not estimate them. In the cases in this CBA where we have not estimated costs or
benefits, this is due to it not being reasonably practicable to do so.
3. This CBA presents our analysis of the expected impacts of a proposal to: create a
directory of specialist
5
travel insurance firms; and to require firms to signpost to this
the harm faced by some consumers with pre-existing medical conditions (PEMCs)
when looking for travel insurance. We provide monetary estimates for the impacts
where we believe we can reasonably estimate them and it is reasonably practicable to
do so. Otherwise, where possible, we provide estimates on the potential number of
consumers affected.
4. The CBA has the following sections:
• Data used and limitations
• Problem and rationale for our Proposal
• Our Proposal
• Baseline and key assumptions
•
•
• Costs
Data used and limitations
5. For the purposes of this CBA we have not conducted a formal data request from firms
in the market. Our Proposal has a relatively small expected cost per firm and we have
already obtained information (both data and qualitative information) from firms during
our Call for Input and engagement with firms.
In these circumstances, we believe
it would not have been proportionate to undertake a formal data request, with the
burden of doing so falling on firms.
with more serious medical conditions.
30 firms on this area of work.
Search

17
CP19/23
Annex 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
6. However, the data we have are limited at times in terms of detail and are from a small
number of firms (8). Whilst we have tried to ensure that the data used represent a
range of different firms with different business models, the limited amount of data
means our estimates are more indicative and sensitive to outliers than they would
otherwise be. We welcome feedback on the estimates we provide.
Problem and rationale for our Proposal
The harm and drivers of harm
7. In our Feedback Statement on our Call for Input on Access to Insurance (FS18/1) we
outlined how it can be difficult for some consumers who have, or have had, cancer
to find affordable travel insurance with appropriate cover. Some responses to the
initial Call for Input and wider feedback from stakeholders suggested that this
harm is not specific to cancer, and that consumers with other PEMCs experience
8. The 3 key harms we identified in FS18/1 and through further engagement with firms
and consumer organisations are that some consumers with PEMCs are:
• not able to obtain insurance
• able to obtain insurance but without cover for their PEMC (i.e. with an exclusion)
•
than they could get elsewhere in the market
9. The main driver of these harms is that consumers with PEMCs lack awareness of
specialist travel insurance firms as well as the potential to remove exclusions for
PEMCs. An additional driver of harm for consumers who may be paying a significantly
higher price is them finding it difficult to assess and compare the value of different
products, for example prices and associated cover between mainstream and
Consumers cannot get cover or can only obtain cover with an exclusion for
theirPEMC
10. In FS18/1 we found that some consumers with PEMCs are not aware that there are
alternative travel insurance firms, which are able to offer insurance to consumers with
the risk appetite of mainstream travel insurance firms, these consumers often cannot
find cover. This can be through not being offered insurance at all, by being offered
insurance that excludes cover for their PEMC or because they are quoted a premium
for insurance that would cover their PEMC which they deem as unreasonably high.
11. Consumers not being able to access cover results in consumer harm as they then
choose between travelling without cover, and bear the financial risk associated with
this, or not travelling at all. The impact of this is not necessarily mitigated by traditional
shopping around, such as using a price comparison website, as most mainstream firms
use a similar approach to medical screening and specialist firms are not always on price
comparison websites. Other consumers may not attempt to shop around as they may
consider a high premium, or a decline to provide cover from a mainstream firm, is a
reflection of their ability to obtain cover more generally.
Search

18
CP19/23
Annex 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
12. Additionally, it is sometimes possible for consumers to remove the exclusion on
their offered policy from the mainstream firm in exchange for an increased premium.
However, consumers are often unaware that this is possible. This can be the case for
travel insurance that comes with packaged bank accounts, where a PEMC exclusion
often comes as standard.
Consumers can obtain cover however pay signicantly more than ecient costs
13. In those cases where mainstream firms are prepared to offer insurance to consumers with
more serious PEMCs, feedback to our work has suggested that in some circumstances,
they may charge a relatively high price, compared to more specialist firms.
14. We understand that this difference in prices offered is due to these individuals being
firms may have limited experience of these risks and do not price the risk as accurately
as more specialist firms, or they may attempt to deter the consumer from purchasing
the policy by offering a very high premium rather than declining the risk.
7
This,
consumers paying higher prices than they could elsewhere for similar levels of cover.
Our Proposals
15. To address the harms identified above, we are proposing to require firms to signpost
some consumers to a directory of firms who specialise in providing cover for PEMCs,
particularly for more serious conditions. The signposting will be required where the
consumer: is declined or not offered cover or has their cover cancelled mid-term; is
offered cover with an exclusion for a PEMC; or offered a policy with additional loading
applied to their base premium due to their PEMC. Firms will be required to indicate
which consumers are more likely to benefit from using it and state the potential
benefits of accessing it.
16. We are working closely with MAPS around the development of the directory to provide
a range of information on specialist firms, such as the types of medical conditions
they cover and how they can be contacted by consumers. Firms listed on the directory
would be validated jointly by the FCA and MAPS, with firms being audited periodically.
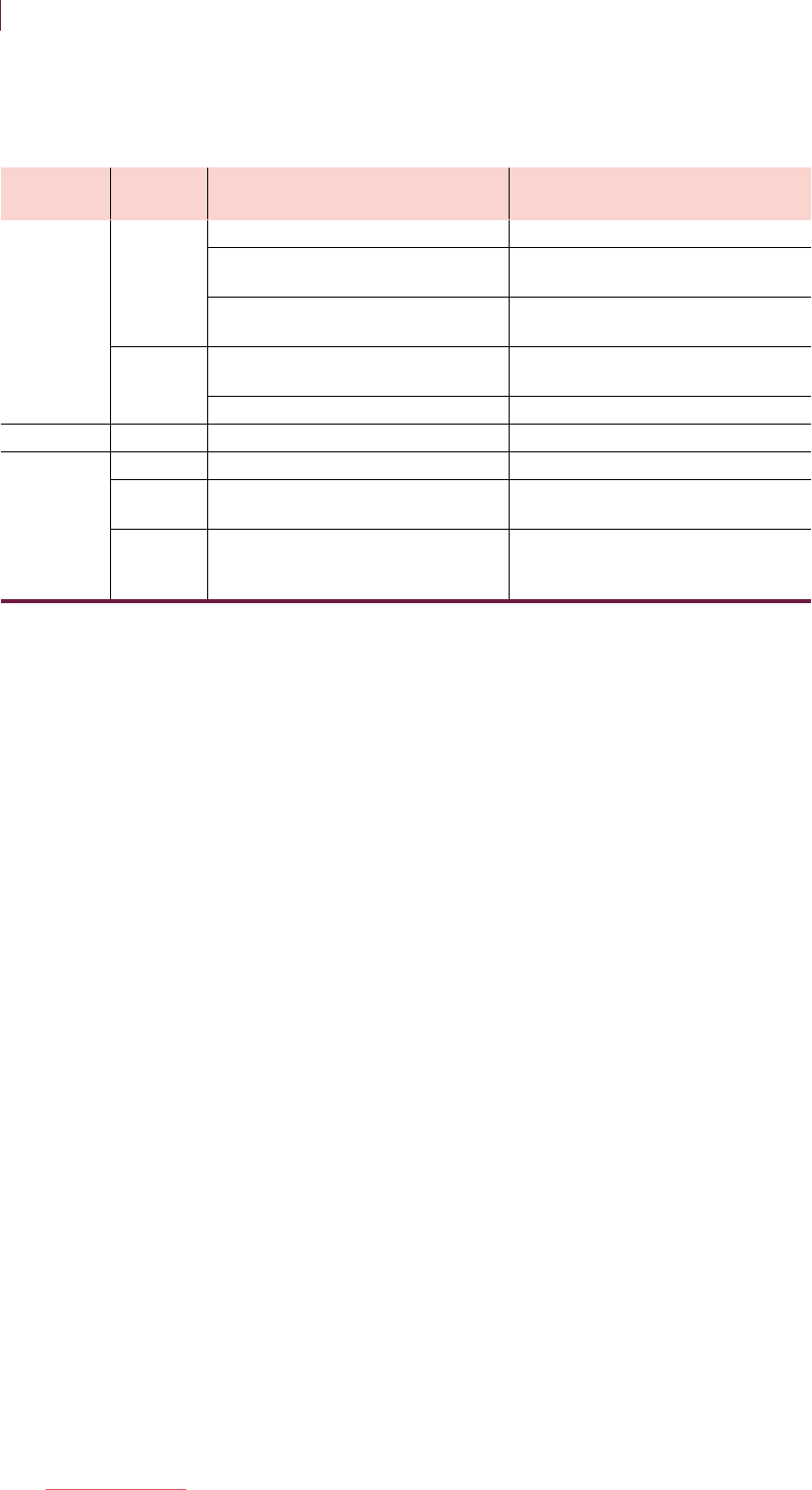
17. Figure 1 outlines how we expect the signposting requirement to improve consumer
outcomes.
7 Firms may be obliged to offer cover up to a certain level of medical condition in order to be shown on a price comparison website.
If the firm does not wish to take on the risk around this medical condition cut-off, one way to do so whilst not contravening their
obligation is to offer a relatively high price.
Search

19
CP19/23
Annex 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Figure 1 – How we expect our Proposal to improve consumer outcomes
MAPS develop a directory of specialist
providers who are better able to cover PEMCs
The FCA requires rms to signpost to the
public directory of specialist providers
Consumers with more serious PEMCs who usually use mainstream rms become more aware of
the presence of specialist providers in the market
Consumers with more serious PEMCs use the public directory to nd specialist providers who
are better suited to cover their PEMC
Consumers who do not receive
oers from mainstream
providers, or can’t aord them,
now seek quotes from
specialist providers
Consumers who only receive
oers which exclude coverage
for their PEMC now seek quotes
from specialist providers
Consumers who receive oers
from mainstream providers
compare these with those
from specialist providers
Increased coverage for
consumers with PEMCs who
previously weren’t able to
obtain coverage
Increased coverage for
consumers with PEMCs who
previously were only able to
obtain coverage with
exclusions
Lower prices for consumers
with PEMCs who previously
paid ‘high’ prices for insurance
from mainstream providers
Consumers who previously did not travel due to lack of cover
now travel, whilst consumers who previously travelled without
cover now travel with cover
18. The signposting requirement will be complemented by proposed guidance to firms
clarifying that, where an exclusion is applied due to a PEMC, firms should inform the
consumer whether the exclusion can be removed and, if so, how this can be done.
Furthermore, additional guidance is proposed setting out FCA expectations for firms
that offer cover to consumers at very high premiums (and that firms should calculate
medical condition premiums by reference to reliable information that is relevant to the
assessment of the risk).
19. It will also be complemented by a package of other proposals, including:
• Working with MAPS to improve consumer understanding of travel insurance policies
their pricing, and reiterate the importance of insurance; and
• Working collaboratively with our stakeholders to improve the wording used in the
medical screening process, aiming to make the journey as easy as possible for
consumers.
20. Further details on the proposals can be found in Chapter 3 of the Consultation Paper.
Search
20
CP19/23
Annex 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Baseline and key assumptions
Baseline
21. The starting point for our baseline is the current level for each of the outcomes we are
interested in improving, as illustrated in Figure 1. Where we hold estimates of these,
we have listed them in Table 1 below. We use these estimates later in the CBA to help
inform our estimates of costs and benefits.
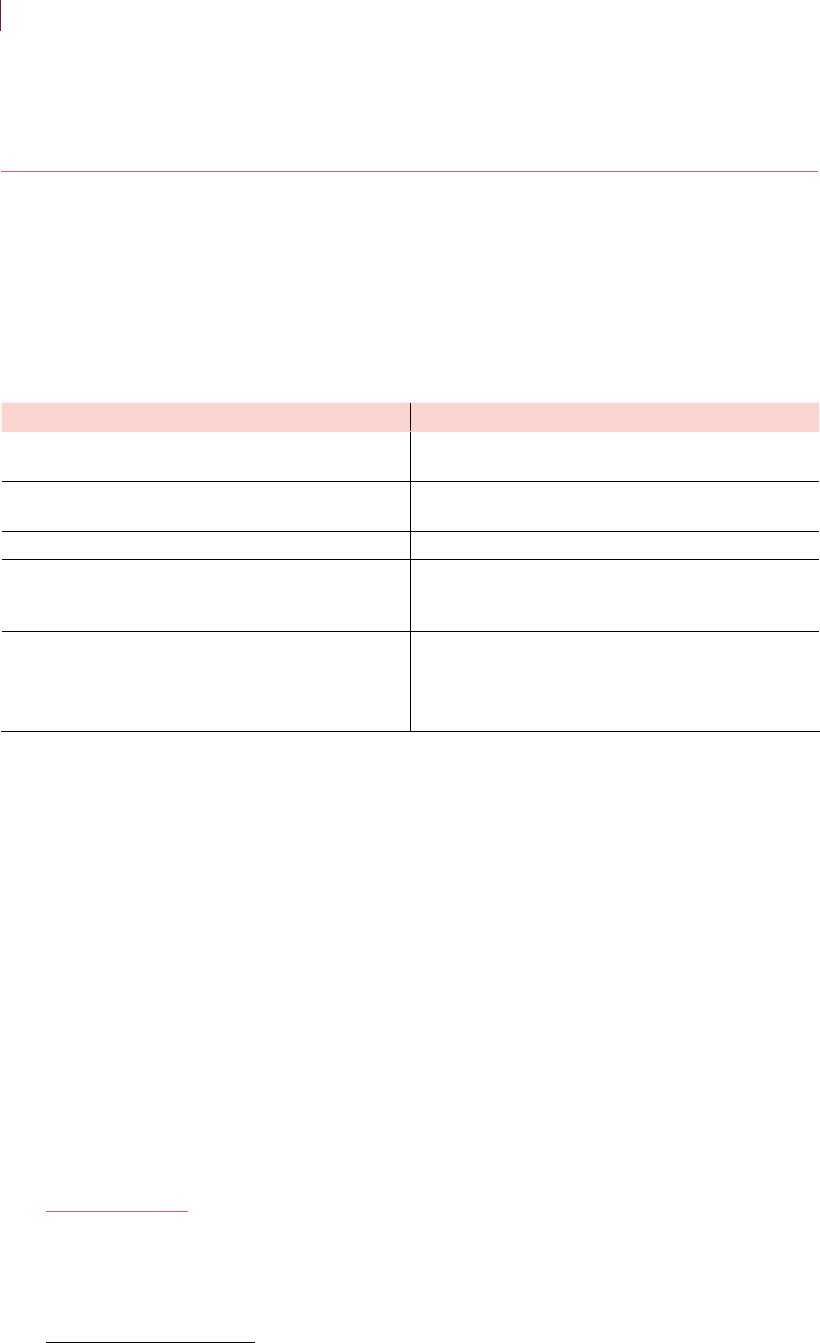
Table 1 – Baseline for key outcomes
8
Outcome of interest Estimate % (and absolute amount)
Consumers who undergo medical screening due to
having a PEMC
9
10
Consumers with PEMCs who have insurance that
excludes cover for their PEMC
11
Consumers declined cover due to a PEMC 0.3% (94,000-105,000)
12
Consumers who have a high
13
medical screening
Proposal
Average premium paid by consumers for insurance
that covers their PEMC
more serious PEMCs: £1,500
serious PEMCs: £900
14
Source: ABI, ONS, Mintel, firm data, FCA calculations
22. Following engagement with firms, we understand that some firms are starting to put
in place arrangements to refer consumers on to more specialist firms where they
are unable to offer cover themselves. This will impact on our baseline, although it is
difficult to estimate by how much. The estimated costs of implementing our proposal
may decrease as the number of firms that are starting to put in place signposting
arrangements increases.
15
However, there will also be an associated decrease in
benefits.
Key assumptions
23. In Table 2 we set out: the main assumptions used when conducting the CBA; their
reasoning; and potential consequences if they do not hold.
24. In our analysis, we have assumed that the firms for which we have data are
representative of the wider market. We have scaled up their data, where possible
and appropriate, based on their size and market share. These firms may not be
8 Numbers presented in the table are rounded. The underlying calculations use un-rounded numbers. Therefore, using the numbers in
the table to re-create estimates may result in small errors.
methodologies to improve the robustness of our estimates. Thus, subsequent calculations based on this number will have a range
that reflects this. This estimate is based on the best information available to us and we welcome feedback on our estimates.
10 Travel Insurance: UK, February 2019, Mintel estimates that around 40% of travel insurance consumers undergo medical screening.
11
This estimate is based on data from a limited number of firms. We believe that it may not fully account for exclusions that apply on
packaged bank accounts. As such, this should be taken as an estimate of the lower bound.
12
This percentage estimate is based on data from 1 large firm. This may include double counting of consumers who are rejected by
more than one firm when seeking cover or who initially seek multi-trip cover but then take single trip cover. As such, it should be
taken as an upper estimate.
13
There are different medical screening firms in the market, who score using different methodologies. As such, we have not listed what
this score would be. However, based on the data provided to us, this captures only the most severe of conditions.
14
These estimates are sourced from only 1 larger firm, thus are highly indicative.
15 If firms are able to implement our proposals at the same time as implementing their own signposting arrangements then we would
expect costs to decrease given the overlap of these two bits of implementation would decrease fixed costs.
Search

21
CP19/23
Annex 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
representative of the wider market and thus we may over or under estimate the costs
and benefits of our Proposal, but we consider this is a reasonable approach to take for
the reasons set out in the “Data used and limitations” section.
Table 2 – Assumptions and rationale
Assumption Rationale
Consequence of
assumption not holding
The travel insurance
market stays the same size
Market research companies estimate that
the market has seen little growth over
the past 5 years and we cannot foresee
anything that might change this
We under or over-estimate
The specialist market
is competitive with no
No evidence was provided to us as part
of our Call for Input that suggested a lack
of competition in the specialist market
was an issue. We also have evidence that
prices in the specialist market are lower
than the mainstream market
Some of the estimated
lower prices will be taken by
The ability of consumers
with PEMCs to access
insurance will not
improve in the absence of
regulatory interventions
We are not aware of any market
developments, or proposed
comprehensive service, that will
consumers with PEMC to access
insurance
of our Proposal
Summary of costs and benefits
25. Table 3 sets out a summary of the main costs and benefits we expect as a result of our
Proposal.
This indicates that market power is not being exploited.
Search

22
CP19/23
Annex 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Table 3 – Summary of costs and benets
One-o/
annual
Costs Benets
Firms
•
£225,000
• Costs of implementing and
complying with our Proposal –
£12.2 million
• Application to directory of
Annual
• Loss of revenue (net of transfers) –
• Costs of implementing and
complying with our Proposal –
• Increased sales to consumers
insurance – Not monetised, but
estimated at 2,700-3,100 sales
• Improved trust in the travel
insurance market – Not estimated
Consumers Annual
• Increased search costs (new
consumers) – Not estimated
•
• Improved cover of PEMCs for those
who already have insurance – Not
consumers)
• Access to cover for those who
consumers)
• Decreased search costs (existing
consumers) – Not estimated
Source: ABI, ONS, Mintel, firm data, FCA calculations
26. Based on the costs and benefits estimated above, as well as the number of consumers
likely to be affected (for the impacts that are not monetised) we can estimate the per-
27. This takes into account that we have already estimated some benefits for consumers
from lower prices paid, which is offset by lost revenue to firms. We estimate this break-
even amount using a 10-year net present value methodology.
17
28. Our break-even analysis estimates that the average benefit per affected consumer
would need to be £90-100 per year to offset the estimated costs of our Proposal over
a 10-year period.
29. Additionally, we note that the consumers we aim to assist with our Proposal have a
pre-existing medical condition. As such, they are more likely to be vulnerable and the
benefits to them of improved cover are likely to be higher than the average consumer.
We also consider the value of the transfer from firms to consumers of reduced prices
to be greater for these consumers, and this would reduce the break-even estimates
above (of £90-100) if we weighted benefits to reflect this.
17 This combines the one-off cost and each of the ongoing costs over the next 10 years, discounted back to their net present value.
To do this we use a discount rate of 3.5%, as recommended by the HMT Green Book. It then compares this against the accumulated
number of expected affected consumers over the 10-year period.
Search

23
CP19/23
Annex 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Benefits
30. Below we set out in more detail the benefits we expect to arise for firms and
consumers. These are all on an ongoing basis. A summary can be found in Table 4
below.
Table 4 – Summary of benets
Benet type Benet estimate (annual)
Firms
Increased sales to consumers who
Not monetised – estimated increase
in sales of 2,700-3,100
Improved trust in the travel insurance
market
Not estimated
Consumers
Lower prices paid by existing consumers
Improved cover of PEMCs for those who
already purchase insurance but with
exclusions for their PEMCs
Increased access to insurance and cover
of PEMCs for those who previously
2,700-3,100 consumers
Decreased search costs for consumers
who already purchase
Not estimated
Source: ABI, ONS, Mintel, firm data, FCA calculations
Benets to rms
31. We expect some firms (e.g. specialist firms) to benefit from increased sales as a result
of our Proposal. However, this benefit will be at the expense of losses to other firms, so
will net out. This is discussed under the “Costs to firms” section.
32.
now purchase insurance as a result of our proposed signposting. This will be a benefit
to firms as these sales previously did not take place. We estimate the potential number
of sales in the “Benefits to consumers” section below. These are estimated at an
additional 2,700-3,100 sales annually.
33. An additional benefit to firms we expect due to our Proposal is improved trust in the
travel insurance market. Consumers being made aware of, and using, specialist firms
that provide them with appropriate cover will decrease the incidence of unexpected
shocks when consumers attempt to claim. This will increase consumers trust in the
travel insurance market and potentially lead to increased purchasing. We have not
attempted to quantify the impact of this as we consider it not practicable to do so.
Benets to consumers
34. We expect the benefits to consumers to all be ongoing. We group these into two main
categories:
1. Lower prices for consumers with PEMCs who are already able to obtain insurance.
2. Increased cover for those who previously were not able to get cover for their PEMC.
35. The estimates we provide below will be higher if the effectiveness of signposting in
getting a consumer with a PEMC to follow through and purchase from a better placed
specialist firm is higher than a 2.9% increase (which is the effectiveness we use in our
estimates).
Search

24
CP19/23
Annex 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
36. We also expect our Proposal to lead to decreased search costs (i.e. saved time) for
those consumers who would have searched for specialist firms irrespective of our
Proposal. However, due to the small size of potential benefits we consider it not
practicable to estimate them.
Lower prices for consumers who already obtain insurance
37.
18
to mainstream firms now pay a lower price for the same level of cover to a specialist firm.
This is a result of these consumers seeing the signposting after being offered a high
price by mainstream firms, going to the directory of specialist firms and then purchasing
38. To estimate this, we use data from Table 1 on the number of consumers who have
more serious PEMCs, and thus are likely to face higher prices, and data we received
from 1 firm on the impact of their own signposting.
20,21
Our data estimates that around
1.1% of consumers have a serious PEMC meaning they are likely to face a high price
from mainstream firms. Data on the impact of signposting estimates that, of those
who are signposted, around 2.9% go on to purchase from the specialist firm
22
at a
price that is around £1,200
23
less than they were originally quoted. Thus, we estimate
prices.
24
This estimate assumes that all consumers with more serious PEMCs currently
purchase from mainstream firms, and is therefore likely to be an upper bound estimate
of these benefits.
39. In addition to the benefits estimated above, there are potential benefits from lower
prices for those with less serious PEMCs. To provide an indication of the size of this
group, 5.5% of consumers (1.7-1.9 million) have a medical screening score where firms
on a price comparison website are not obliged to offer cover.
25,
However, we would
expect the effectiveness of the signposting, and savings available per consumer, to
decrease as the severity of the PEMC decreases. It is not practicable to estimate these
potential benefits with a reasonable degree of accuracy.
18 Feedback to our work suggests that some consumers with more serious PEMCs can face relatively high prices from some
mainstream firms when compared to specialist firms. This was not suggesting mainstream firms are exercising market power, rather
they have different risk modelling approaches and tolerances.
19
See row 4.
20 We cannot provide further information on the firm for confidentiality reasons, however we have no reason to believe that the data
provided to us is not representative of the broader market.
21
The data provided is on the effectiveness of a firm signposting to a specialist firm where the offered premium to a consumer with a
PEMC is above a given threshold. This is likely to correspond with the consumer having a more serious PEMC.
22
The small proportion that go on to purchase from the specialist firm is small due to only a small number going through the medical
screening process with the specialist firm (around 10% of those who see the signposting). Around 50% of those who follow the
signposting and undergo medical screening are offered coverage.
23
This is based on data from 1 firm who conducts their own signposting.
24
x effectiveness of signposting (2.9%) x saving from purchasing policy from a specialist firm (£1,200)/average number of consumers
per policy (1.7).
25
For a firm to sell through a price comparison website, they are usually required to offer coverage for consumers who have a medical
screening score below a given level. We think that consumers with scores above this level will be more likely to benefit from our
Proposal.
This includes those with more serious PEMCs.
Search

25
CP19/23
Annex 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Increased cover for consumers who previously did not have cover for their
PEMC
40. We expect consumers to benefit from increased cover in the following ways:
a. Consumers who previously purchased insurance from a mainstream provider with
an exclusion on their PEMC now purchase insurance with cover for their PEMC after
being signposted to the directory of specialist providers.
b.
41. We are unable to monetise these benefits due to data limitations and it not being
practicable for us to do so. We do not have data on: consumers travelling with an
exclusion on their PEMC; consumers choosing not to travel due to the exclusion; how
many consumers were not offered cover; or how many consumers could not afford the
offered cover.
42. However, we can estimate how many consumers we think will be affected by our
Proposal and thus stand to benefit.
43. For a), we estimate 11.2%
27
on their policy for their PEMC. If our proposed signposting has the same impact as it
has on those who face a relatively high price (i.e. 2.9% respond), then we would expect
excluded from their cover.
44. For b), we estimate around 0.7%
28
of consumers with a PEMC (94,000-105,000) are
not offered cover. If our proposed signposting has the same impact as it has on those
who face a relatively high price (i.e. 2.9% respond), then we would expect 2,700-3,100
consumers to benefit annually from now being able to access cover.
Costs
45. Below we set out the costs we expect to arise for firms, consumers and the Money and
Pensions Service (MAPS) on a one-off and ongoing basis. A summary can be found in
Table 5 below.
27 This is estimated using data from 2 firms who provided information on sales and exclusions. Based on feedback to our work in this
area, we expect this percentage to be higher given the number of packaged bank accounts and the fact that they normally come
with an exclusion for PEMC coverage as standard.
28
This is estimated using data from 1 firm. This firm has a significant market presence. Additionally, we have benchmarked this piece of
data against ad hoc data provided by smaller firms in the market.
Search
CP19/23
Annex 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Table 5 – Summary of costs
One-o/
ongoing
Cost type Cost estimate
Firms
£225,000
Rule implementation costs (i.e. IT
changes, training, governance)
£12 million
Application to directory of specialist
Minimal
Ongoing
Rule implementation costs (i.e. IT
changes, training, governance)
£4 million
Loss of revenue (net of transfers)
Consumers Ongoing Increased search costs Not estimated
MAPS
Development of directory Within existing resources
be on the directory
Within existing resources
Ongoing
the directory and validation of new
entrants
Within existing resources
Source: ABI, ONS, Mintel, firm data, FCA calculations
Costs to rms
46. We consider both one-off and ongoing costs to firms. For our cost estimates, we have
received data from 4 firms to estimate the impact on larger firms, whilst information
from a trade body suggests the costs faced by smaller firms will be minimal.
47. Using our understanding of the market, and information received as part of our Call for
Input, we estimate there to be around 130 larger firms in the market.
One o costs
48. There will be costs to firms to familiarise themselves with the new rules and conduct
estimator tool to estimate these for all firms in the market (both large and small). We
estimate these at £225,000.
49. We also expect firms to incur IT, staff training, sales process and documentation
change costs to update their systems and documents to be compliant with our new
rules, and ensure their frontline and phone staff are appropriately implementing them.
Applying the average of cost estimates provided by 4 firms to the 130 firms, we expect
these to be around £12.2 million.
29
50. For specialist firms specifically, we expect there to be a time cost associated with
applying to be admitted to the directory. However, we expect this cost to be minimal
when considered in the context of their broader compliance and governance
processes.
Ongoing costs
51. We expect firms to incur ongoing staff training, longer documentation and increased
frontline staff costs associated with our Proposal. Applying the average of cost
estimates provided by 4 firms to the 130 firms, we expect these to be around £4 million
annually.
29 The average estimated one-off cost for a large firm is £94,000. This will vary by firm type, size and business model.
Search

27
CP19/23
Annex 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
52. We expect some firms (mainstream firms who do not specialist in PEMCs) will lose
revenue as result of our Proposal. However, some of this will be a transfer to other
firms (those who specialise in PEMCs) whilst the remainder of this will be a transfer to
consumers in the form of lower prices.
53. We estimate the net cost to firms. This is the lost revenue, once adjusting for gains
to some firms. As discussed in the “Benefits to consumers” section, we expect
our proposed signposting requirement to lead to some consumers who previously
purchased from mainstream firms to now purchase from more specialist firms. As
specialist firms offer a given level of cover for a lower price for those with more serious
PEMCs, this will lead to an overall decrease in the revenue of firms.
54. This decrease in net revenue for firms will be equal in magnitude to the benefit to
consumers from lower prices estimated above. To estimate this, we use our estimate
from the “Benefits to consumers” section on the benefits to consumers from lower
in that section, the true cost to firms could be lower if a large number of consumers
with serious PEMCs already purchase from specialist firms whilst it could be higher if
consumers with less serious PEMCs also take advantage of the signposting.
55. Additionally, we expect that the signposting to the directory of specialist firms will lead
to some consumers who previously would have purchased cover with an exclusion for
their PEMC from a mainstream firm to now purchase cover without an exclusion from a
specialist firm.
56. It is difficult to estimate the impact this will have on overall firm revenues as consumers
may pay more but for a higher level of cover or less for a similar level of cover. As such,
it is not practicable to estimate the impact of this.
Costs to consumers
57. We expect there will be ongoing costs to consumers but no one-off costs.
58.
spend more time shopping around, discussing their medical condition and needs, and
comparing cover. We have not estimated this as the additional time will be specific to
Costs to MAPS
59. We expect there to be some one-off resource costs for MAPS in developing the
directory and in validating firms who want to be on the directory. We expect there to be
ongoing resource required to validate new entrants to the market and periodically audit
those already on the directory.
60. We expect these costs to be met by MAPS from within their current budget. The FCA
will assist MAPS with this process, with this also met from within our current resourcing.
Search

28
CP19/23
Annex 2
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Annex 3
Compatibility statement
Compliance with legal requirements
1.
reasons for concluding that our proposals in this consultation are compatible with
certain requirements under the Financial Services and Markets Act 2000 (FSMA).
2. When consulting on new rules, the FCA is required by section 138I(2)(d) FSMA to
include an explanation of why it believes making the proposed rules is (a) compatible
with its general duty, under s. 1B (1) FSMA, so far as reasonably possible, to act in a
way which is compatible with its strategic objective and advances one or more of its
operational objectives, and (b) its general duty under s. 1B(5)(a) FSMA to have regard
to the regulatory principles in s. 3B FSMA. The FCA is also required by s. 138K (2) FSMA
to state its opinion on whether the proposed rules will have a significantly different
impact on mutual societies as opposed to other authorised persons.
3.
the duty on the FCA to discharge its general functions (which include rule-making) in
a way which promotes effective competition in the interests of consumers (s. 1B (4)).
This duty applies in so far as promoting competition is compatible with advancing the
4. In addition, this Annex explains how we have considered the recommendations made
by the Treasury under s. 1JA FSMA about aspects of the economic policy of Her
duties.
5. This Annex includes our assessment of the equality and diversity implications of these
proposals.
6.
determining general policies and principles and giving general guidance (but not when
exercising other legislative functions like making rules). This Annex sets out how we
have complied with requirements under the LRRA.
Search

29
CP19/23
Annex 3
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
The FCA’s objectives and regulatory principles: Compatibility
statement
7.
market integrity objectives.
8. Our proposals are designed to improve the way the travel insurance market operates
by:
• Protecting consumers with PEMCs – by providing information about the availability
of travel insurance for consumers with PEMCs this will improve access to travel
insurance, reducing the number of uninsured consumers and consumers travelling
with exclusions for PEMCs
• Increasing market integrity – by enabling more consumers with PEMCs to access
9.
ensuring that the relevant markets function well because our proposals will improve
strategic objective, “relevant markets” are defined by s. 1F FSMA.
10. In preparing the proposals set out in this consultation, the FCA has had regard to the
regulatory principles set out in s. 3B FSMA.
The need to use our resources in the most ecient and economic way
11. We have worked closely with a range of stakeholders to identify a solution to improve
access to travel insurance for consumers with PEMCs. We are working closely with
MAPS around the development of the directory of providers and consider this to be
the most efficient and economic way for the directory to be set up.
The principle that a burden or restriction should be proportionate to
the benets
12. By working closely with stakeholders, we have sought to ensure, as far as possible, that
the burden to firms is proportionate to the benefits. However, in some cases we have
not estimated costs of benefits where we consider it is not reasonably practicable to
do so.
The desirability of sustainable growth in the economy of the United
Kingdom in the medium or long term
13. We do not consider that the proposals are inconsistent with this principle, and they are
expected to increase the number of consumers with PEMCs who purchase appropriate
travel insurance.
The general principle that consumers should take responsibility for
their decisions
14. Our proposals are consistent with the principle that consumers should take
responsibility for their decisions, but rather provide affected consumers with more
information to make more informed decisions about choosing travel insurance.
Search

30
CP19/23
Annex 3
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
The responsibilities of senior management
15. Our proposals do not impact on the responsibilities of senior management.
The desirability of recognising dierences, and objectives of,
businesses carried on by dierent persons including mutual societies
and other kinds of business organisation
16. We do not believe that our proposals discriminate against any particular business
model or approach in the travel insurance market. There is wide support across
different businesses to take action to improve access to travel insurance.
The principle that we should exercise of our functions as transparently
as possible
17. We believe that by consulting on our proposals we are acting in accordance with this
principle.
18. In formulating these proposals, the FCA has had regard to the importance of taking
action intended to minimise the extent to which it is possible for a business carried on
(i) by an authorised person or a recognised investment exchange; or (ii) in contravention
of the general prohibition, to be used for a purpose connected with financial crime (as
required by s. 1B(5)(b) FSMA).
Expected effect on mutual societies
19. The FCA does not expect the proposals in this paper to have a significantly different
impact on mutual societies. We have worked with mutual societies through our
engagement with stakeholders to develop and refine our proposals.
Compatibility with the duty to promote effective competition
in the interests of consumers
20. In preparing the proposals as set out in this consultation, we have had regard to the
that by signposting consumers with PEMCs to a directory of more specialist providers,
competition for some consumers with PEMCs may increase.
21. We expect this as, under our proposal, consumers with PEMCs will be directed to a
directory where they can find, and subsequently compare offers from, a larger range
Equality and diversity
22. We are required under the Equality Act 2010 in exercising our functions to ‘have
any other conduct prohibited by or under the Act, advance equality of opportunity
between persons who share a relevant protected characteristic and those who do not,
Search

31
CP19/23
Annex 3
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
to and foster good relations between people who share a protected characteristic and
those who do not.
23. As part of this, we ensure the equality and diversity implications of any new policy
proposals are considered. The outcome of our consideration in relation to these
matters in this case is stated in paragraph [2.9] of the Consultation Paper.
Legislative and Regulatory Reform Act 2006 (LRRA)
24. We have had regard to the principles in the LRRA for the parts of the proposals that
consist of general policies, principles or guidance. We consider that our proposal is:
• Transparent: We are consulting on our proposed rules and guidance
• Accountable: By consulting we are seeking feedback on our proposed approach
• Proportionate: We consider that our proposals are proportionate and have sought
to minimise costs to achieve the outcomes we are seeking
•
• Targeted only at cases in which action is needed: Our proposed signposting targets
improved access to insurance.
25.
of general policies, principles or guidance. We consider that the proposals will be
effective in helping firms understand and meet regulatory requirements more easily,
in a manner that leads to improved outcomes for consumers and addresses the issues
identified in this market.
Search

32
CP19/23
Annex 3
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Annex 4
Abbreviations used in this paper
CBA Cost Benefit Analysis
CfI Call for Input
CP Consultation Paper
FS Feedback Statement
LRRA
MAPS Money and Pensions Service
PBA Packaged Bank Accounts
PEMCs Pre-existing medical conditions
We have developed the policy in this Consultation Paper in the context of the existing UK and EU
regulatory framework. The Government has made clear that it will continue to implement and apply
EU law until the UK has left the EU. We will keep the proposals under review to assess whether any
amendments may be required in the event of changes in the UK regulatory framework in the future.
We make all responses to formal consultation available for public inspection unless the respondent
request for non-disclosure.
Act 2000. We may consult you if we receive such a request. Any decision we make not to disclose the
response is reviewable by the Information Commissioner and the Information Rights Tribunal.
All our publications are available to download from www.fca.org.uk. If you would like to receive this
or write to: Editorial and Digital team, Financial Conduct Authority, 12 Endeavour Square, London
E20 1JN
Search

33
CP19/23
Annex 4
Financial Conduct Authority
Signposting to travel insurance for consumers with medical conditions
Appendix 1
Draft Handbook text
Search
FCA 2019/XX
INSURANCE: CONDUCT OF BUSINESS SOURCEBOOK (ACCESS TO
TRAVEL INSURANCE) INSTRUMENT 2019
Powers exercised
A. The Financial Conduct Authority (“the FCA”) makes this instrument in the exercise
of the powers and related provisions in or under:
(1) the following sections of the Financial Services and Markets Act 2000 (“the
Act”):
(a) section 137A (The FCA’s general rules);
(b) section 137T (General supplementary powers);
(c) section 139A (Power of the FCA to give guidance); and
(2) the other powers and related provisions listed in Schedule 4 (Powers
exercised) to the General Provisions of the Handbook.
B. The rule-making powers listed above are specified for the purpose of section 138G
(Rule-making instruments) of the Act.
Commencement
C. This instrument comes into force on [date].
Amendments to the Handbook
D. The Glossary of definitions is amended in accordance with Annex A to this
instrument.
E. The Insurance: Conduct of Business sourcebook (ICOBS) is amended in accordance
with Annex B to this instrument.
Citation
F. This instrument may be cited as the Insurance: Conduct of Business Sourcebook
(Access to Travel Insurance) Instrument 2019.
By order of the Board
[date]
FCA 2019/XX
Page 2 of 7
Annex A
Amendments to the Glossary of definitions
Insert the following new definitions in the appropriate alphabetical positions. The text is not
underlined.
medical condition
exclusion
an exclusion in respect of one or more medical conditions.
medical condition
premium
any amount of premium relating to the risk associated with one or more
specific medical conditions.
medical cover firm
directory
a publicly available directory:
(a) that lists firms that provide or arrange travel insurance policies
that cover more serious medical conditions;
(b) that does not prevent firms from being listed based on any
membership of any association;
(c) that provides detailed information about each listed firm,
including:
(i) the name and contact details of the firm;
(ii) whether it specialises in covering any specific medical
conditions;
(iii) any specific medical conditions that the firm is likely not
to cover;
(iv) any age limits;
(v) whether the firm can discuss medical conditions with
consumers either online or by phone;
(vi) whether the firm can offer cover to consumers who are
currently undergoing treatment;
(vii) whether the firm can offer cover to consumers with a
terminal prognosis;
(d) where the operator verifies the information in (a) and (c) and
keeps the information up-to-date.
travel insurance
policy
(in ICOBS 6.1.7-AG, ICOBS 6.5.1AG and ICOBS 6A.4 (Travel
insurance and medical conditions)) a non-investment insurance
FCA 2019/XX
Page 3 of 7
contract which covers risks connected with travelling or the making of
travel arrangements, including connected travel insurance contracts.

FCA 2019/XX
Page 4 of 7
Annex B
Amendments to the Insurance: Conduct of Business sourcebook (ICOBS)
In this Annex underlining indicates new text, unless otherwise stated.
1 Annex 1 Application (see ICOBS 1.1.2R)
…
Part 2: What?
Modifications to the general application rule according to type of firm
…
5 Travel insurance contracts
5.1 R The provisions in ICOBS 6.1.7-AG, ICOBS 6.5.1AG and ICOBS 6A.4 apply to
all incoming firms (including those providing cross border services) other than:
(1) an incoming firm in respect of that part of its business that was carried
on as an electronic commerce activity from another EEA State; or
(2) an incoming firm where the state of the risk is an EEA State to the extent
that the EEA State in question imposes measures of like effect.
…
5 Identifying client needs and advising
5.1 General
…
Eligibility to claim benefits: policies arranged as part of a packaged bank account
…
5.1.3
C
R …
(3) The statement (provided under ICOBS 5.1.3CR(1)) must not:
(a) include any information other than that required under this rule,
ICOBS 6.1.7-AG and ICOBS 6A.4.3R; or
…

FCA 2019/XX
Page 5 of 7
…
6 Product Information
6.1 Providing product information to customers: general
…
Appropriate information regarding medical condition exclusions in travel insurance
policies
6.1.7-
A
G When a firm provides a consumer with:
(1) a quotation for a travel insurance policy; or
(2) a statement (provided under ICOBS 5.1.3CR (1)) in respect of a travel
insurance policy included in a packaged bank account,
then the firm should disclose to the consumer whether any medical condition
exclusion can be removed from the policy (in whole or in part) and, if so, how,
and the terms on which, it can be removed. Firms are also reminded of their
obligations in ICOBS 5.2.2BR to ensure the policy is consistent with the
consumer’s insurance demands and needs.
Appropriate information for commercial customers
6.1.7
A
G …
…
6.5 Renewals
Renewals
6.5.1 R …
6.5.1
A
G Where a firm proposes to a consumer the renewal of a travel insurance policy,
the firm should provide the consumer with information about whether any
medical condition exclusion can be removed from the policy (in whole or in part)
and, if so, how, and the terms on which, it can be removed. Where one of the
circumstances in ICOBS 6A.4.4R applies, the firm should also provide the
consumer with the additional information specified in ICOBS 6A.4.3R. Firms are
also reminded of their obligations in ICOBS 5.2.2BR to ensure the policy
proposed is consistent with the consumer’s insurance demands and needs.
…
FCA 2019/XX
Page 6 of 7
Insert the following new section, ICOBS 6A.4, after ICOBS 6A.3 (Cross-selling). The text is
not underlined.
6A.4 Travel insurance and medical conditions
Application
6A.4.1 R This section applies in relation to a travel insurance policy, which is not:
(1) a group policy; or
(2) a policy entered into by a commercial customer.
Purpose
6A.4.2 G The purpose of this section is to improve access for consumers to travel
insurance policies that include cover for medical conditions.
Additional pre-contract information for the consumer
6A.4.3 R Where one or more circumstances in ICOBS 6A.4.4R applies, a firm must
communicate in a clear and accurate manner and on paper or another durable
medium in accordance with ICOBS 4.1A:
(1) the details of the medical cover firm directory; and
(2)
the potential benefits of accessing the medical cover firm directory and
which consumers are more likely to benefit from using it to search for
an alternate travel insurance policy.
6A.4.4 R The circumstances in ICOBS 6A.4.3R are where a consumer notifies (or has
previously notified) a firm of a medical condition and a firm:
(1) declines or otherwise does not offer the consumer a quotation, due
(wholly or partly) to the medical condition;
(2) cancels the consumer’s policy due (wholly or partly) to the medical
condition;
(3) offers a policy with a medical condition exclusion which cannot be
removed from the policy;
(4) offers a policy with a medical condition premium;
(5) is the insurance intermediary responsible for communicating any of the
above to the consumer; and/or
(6) is not able to ascertain whether any amount of premium is a medical
condition premium.
6A.4.5 G The FCA considers that [website link TBC] is a medical cover firm directory.
FCA 2019/XX
Page 7 of 7
6A.4.6 G For the purposes of ICOBS 6A.4.3R(2), an example is that a consumer is likely
to benefit from searching the medical cover firm directory where the medical
condition is serious or falls within a medical condition exclusion in the policy.
Responsibility for producing and providing additional information as between insurers
and insurance intermediaries
6A.4.7 G The obligations in this section apply to intermediaries and insurers and the
language of relevant provisions should be construed accordingly. Firms should
still comply with the other rules in ICOBS such as the production and provision
of product information (see ICOBS 6.-1) relevant to the information
requirements in ICOBS 6A.4.3R. Where an insurer is an incoming firm (see
ICOBS 1 Annex 1 (Part 2) 5.1R).
Assessment of medical condition risk
6A.4.8 G (1) Firms should assess the risk associated with medical conditions and
calculate medical condition premiums by reference to reliable
information that is relevant to the assessment of the risk. Firms which
do not do this may therefore communicate unclear, unfair or misleading
price information to consumers and so risk breaching Principles 2, 6
and/or 7, and ICOBS 2.2.2R and/or ICOBS 2.5-1R. Firms also need to
consider their obligations under the Equality Act 2010.
(2) Firms are also reminded of their obligations in PROD 4.2 or 4.3 to
identify and distribute travel insurance policies to the target market.
(3) Prior to a firm offering a policy with a very high medical condition
premium, the firm should take all reasonable steps to consider whether:
(a) the nature of the firm’s medical screening or assessment
process is insufficient to provide a relevant assessment of the
risk, based on reliable information, associated with the
particular medical condition; or
(b) the high premium is intended to indicate an unwillingness to
accept the risk by the firm; or
(c) the high premium is due to the medical condition falling
outside of the firm’s risk appetite or target market.
(4) Where this is the case, offering a quote may mislead the consumer
and/or result in them not being treated honestly, fairly and
professionally in their best interests. Firms should consider instead
whether it would be more appropriate not to offer a quote for the risk,
explain the reason/s why not to the consumer and provide them with the
details of the medical cover firm directory under ICOBS 6A.4.3R.

© Financial Conduct Authority 2019
12 Endeavour Square London E20 1JN
Telephone: +44 (0)20 7066 1000
Website: www.fca.org.uk
All rights reserved
